Chloe’s Case Study // Journey to Ulcerative Colitis and Biologics, Steroids and Back
This is a fascinating and inspiring account that involves Ulcerative Colitis and Biologics medications.
Chloe had been unwell for 18 months prior to contacting us. She was in her mid-twenties and was understandably upset and worried about having been diagnosed with Ulcerative colitis, an Inflammatory Bowel Disease.
From the ‘CDC: The Centre for Disease Control and Prevention’:
“Ulcerative colitis (UC) is the most common type of inflammatory bowel disease (IBD). It affects the inner lining of the colon and rectum, causing complete damage to the lining. People with UC often experience blood or mucous in their stool (poop) and feel an urgent need to empty their bowels.”
PRE Symptoms / Health Challenges
We can see the ‘classic’ Ulcerative Colitis symptoms that Chloe had been experiencing, but in addition, the other areas that had been affected too.

From a Functional Health perspective we are not there to make a medical diagnosis or advise her on how to treat a medical condition.
So whilst this case study is looking at Ulcerative Colitis and Biologics medications – We are looking at the body as a whole and looking to understand how it is working as a system of interconnected systems.
Can we investigate and assess the function of the various systems of her body. And from that insight, explore options of how to enhance the vitality and function.
How do these pieces of the puzzle go together and how are the dots connected? Are any of these health challenges linked to one another?
The ‘Functional’ Remit
Whilst there are certain principles of human function that drive the ‘functional health’ approach, there are certain aspects that by design, are most definitely outside it’s scope and remit.
It doesn’t diagnose or name a condition.
And therefore no prescribed treatment for said condition.
This is a Medical and Allopathic remit and model.
Therefore, the focus is on an integration of approaches to create a safe and effective process. What we focus on is clarifying and assessing the mechanisms, consider the drivers and what may optimise the function.
We’ll see through this case study great examples of the value, support and challenges of both approaches!
Timeline of Chloe’s Ulcerative Colitis and Biologics Experience
The onset of the IBD (Inflammatory Bowel Disease) symptoms seemed to occur quite quickly initially for Chloe.
She was quite unclear of the causes at the time and her Medical Team focussed solely on treating the symptoms and markers of inflammation.
First she tried Mesalazine Suppositories (NHS: Mesalazine), which did not appear to lead to improvements.
Next – a major challenge to her situation was that there was a miscommunication between departments and she received no Medical IBD support during the duration of her pregnancy with her first child.
The birth was traumatic and accompanied by a flare-up of Ulcerative colitis and hospitalisation.
The Medical support was engaged again and further investigations of a Colonoscopy and Biopsies revealed a chronic ulcerative colitis in multiple sections of the colorectal mucosa.
Treatment at this point was ramped up to Intravenous Steroids for 3 days and Oral Prednisone.
The Azathioprine was stopped due to causing Pancreatitis.
Whilst this helped to stabilise the symptoms over the next few months, she still experienced a Hospitalisation with a flare-up.
Hence she needed further support for her Ulcerative Colitis and Biologics were the next consideration. She had a work-up and started on Infliximab Infusions and stopped the Steroids.
That brings us to the point at which Chloe contacted us at the Functional Health Clinic.
She was satisfied that her condition had been diagnosed and was being managed. But she did have some concerns around ongoing treatments, goals beyond the current situation and questions that nobody else was asking and answering.
“My goals are to improve the quality of my life, understand the triggers and how to reduce and manage them. And hopefully aim for remission”.
Opportunities to Optimise
This is why we work with our clients. We carefully consider whether there are any opportunities to optimise the function of the body. Can we assess and create more clarity than the person already has? Are there safe and effective steps that could be applied? What role could we play in the person’s ability to progress towards the goal? Would we add any value?
Sometimes all we need to do is look at the timeline, as above.
It may sound overly simplistic, but so far there had been no investigation into what may be causing the inflammation in the bowels. And no advice had been given beyond the diagnosis of Ulcerative Colitis and Biologics prescription Medications.
So far the advice and prognosis had been that she would require Medical Treatment for the rest of her life.
Yes, there may be genetic elements to this. But DNA coding and genes are not static. There are many factors involved in the expression of gene function. Furthermore, if we actually assess the genetic markers, that will only inform and empower what choices and changes to make.
But – what if there were actual drivers of inflammation in Chloe’s body and colon? Pathogens, toxins, foods, allergens etc?
Ulcerative Colitis is Autoimmune. So are there any factors creating autoimmune mechanisms? Can they be identified and modulated?
Any nutrient deficiencies? Nutrient and toxin excess?
What about gut function beyond levels of inflammation? Ability to digest/breakdown foods, gut toxicity, microbiome balance, intestinal permeability etc?
What about energy pathways, metabolism and thyroid function?
Read on if you want to see what we found out!
There is no skewed or delusional idea that there is a ‘miracle cure’, to what degree something can be improved or whether there will or won’t be ongoing inflammatory/autoimmune factors for Chloe to manage.
But assumptions and presumptions go both ways. Was there anything to say that Chloe could not significantly improve her wellbeing, quality of life and function?
Did she really need to feel so stuck and accept the current opinions on the matter?
The number of ‘stones that can be turned over’ is actually extensive. Someone may choose not to turn them all over, but is important to know they exist.
We don’t know all the answers before working with someone, but we are willing to put a process in place that asks the questions to move towards them.

AutoImmune and Inflammatory Mechanisms
Functionally – we are focussed on understanding more about the inflammatory and autoimmune mechanisms. What could contribute to this and what could resolve it? Being diagnosed with Ulcerative Colitis and Biologics being prescribed to treat it wasn’t fully satisfying for Chloe.
That’s why one of the first tests we ran with Chloe was a Comprehensive Gut Health Test, called the GI Map.
This test will assess many factors and functions in the Gastrointestinal Tract. And so far the only information we had on the GI System was from the Colonoscopy, biopsies and a stand-alone Calprotectin Test.
Here’s a summary of what we found out: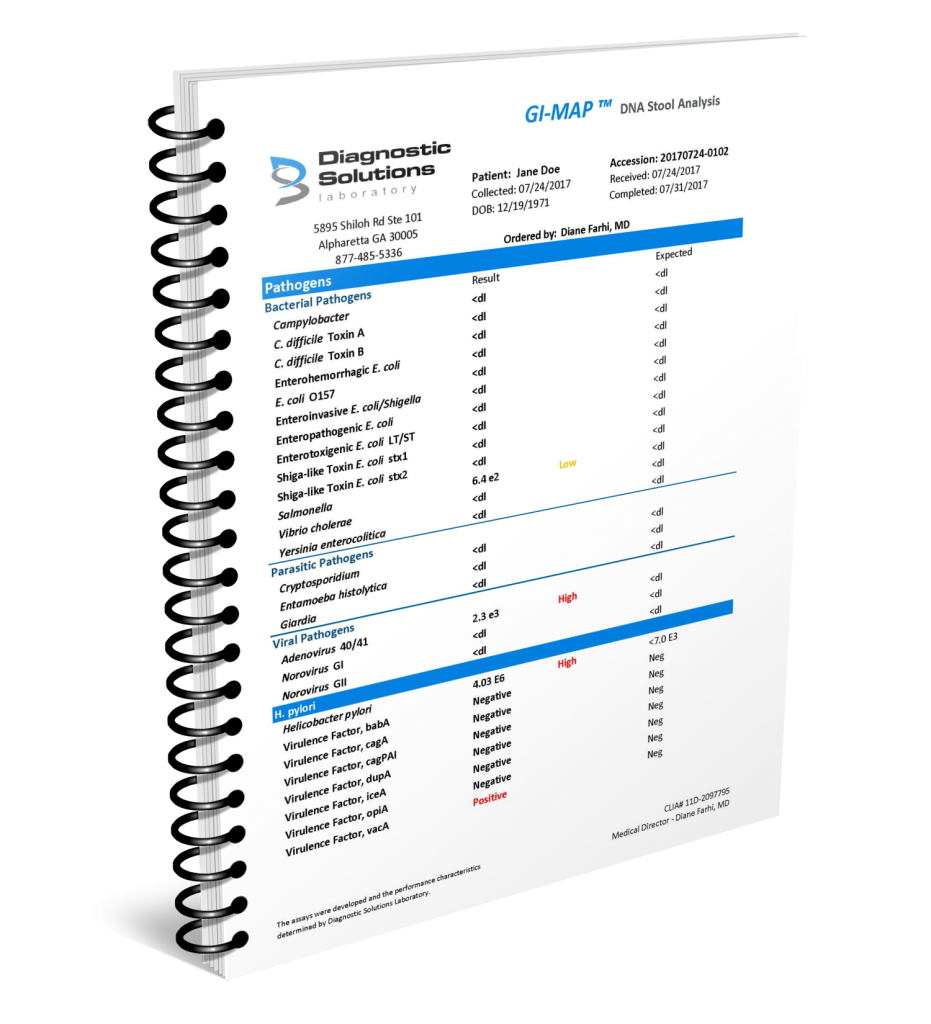
- Enterohemorrhagic E. coli infection
- Microbiome – Diminished Commensal Flora
- Opportunistic Parasite Dientamoeba fragilis
- Digestive Capacity looked normal
- Immune Eosinophil Activation Protein Very High
- Calprotectin Inflammatory marker was High
- Intestinal Permeability
Ulcerative colitis and Enterohemorrhagic E. coli infection

Given that there had not yet been any real investigation into Chloe’s questions of ‘why’ she had Ulcerative colitis, the Enterohemorrhagic E.coli infection discovery was pivotal.
We may have found a chronic level of infection.
As described by the Diagnostic Solutions Lab – ‘Escherichia coli is a large and varied species of bacteria that includes many strains. They colonize humans and animals and are spread through contaminated water, food (undercooked beef, raw milk, and unpasteurized juice) or contact with infected humans or animals. E. coli can cause infections outside of the GI tract such as urinary tract infections, meningitis, and intra-abdominal abscess.’
While there are many harmless, and even beneficial E.coli strains, there are six strains that are notorious for their pathogenicity, especially for GI infections.
Most importantly in Chloe’s case – Enterohemorrhagic E. coli can lead to hemorrhagic colitis or hemolytic uremic syndrome and colonize the colon while the others colonize the small intestines. Acute Symptoms include fever, abdominal cramping, fatigue, nausea, blood and mucus in the stool and diarrhea.
Furthermore there are several factors that make this strain of E.coli particularly Virulent making it both a challenging infection and difficult to eradicate (https://pmc.ncbi.nlm.nih.gov/articles/PMC3710334/)
It wasn’t clear at the time why no tests for pathogenicity of this nature had not already been performed.
Hemolytic Uremic Syndrome (HUS), Ulcerative Colitis and Biologics
Perhaps even more challenging than the actual presence of the pathogen is actually the fact that Enterohemorrhagic E.coli can cause something called Hemolytic Uremic Syndrome.
This scientific review connects some of the dots between the bacterial infection, the HUS and the onset of IBD: https://pmc.ncbi.nlm.nih.gov/articles/PMC6502198/
HUS is a complex condition where the body’s immune system reacts to toxins released during an intestinal bacterial infection. This causes damage and destruction to blood cells as they circulate through the blood vessels.
(More on this later as an Iron Status pattern emerges).
With HUS, the kidney is affected in two ways. The immune reaction can cause direct damage to kidney cells resulting in kidney injury. Alternatively, a build-up of destroyed RBCs or platelets can clog up the kidney’s filtering system and cause kidney injury or a build-up of waste products in the body, since the kidney can no longer efficiently eliminate waste from the blood.
So we can see how the initial infection can have acute symptoms – and the after-effects can potentially have a chronic impact on our function and wellbeing.
As well as ensuring Chloe’s Medical Team were informed and able to provide work-up/monitoring, we also knew that some vital assessments via a comprehensive blood chemistry would help assess aspects of kidney function, inflammation, toxicity and immune function.
Imagine having inflamed bowels but being unaware that there was a virulent E coli bacterial infection and potential for damage, toxicity and kidney challenges in the form of HUS!
Catch-22 or Leverage
On one hand it is a breakthrough of sorts to identify a potentially key piece of the puzzle. Yet with this particular bacterial infection, the conventional Medical treatment of Antibiotics is actually contraindicated due to the increased risk of HUS! The same goes for botanical antimicrobials too.
Rather than perceiving this as a catch-22, in these situations at the Functional Health Clinic we are always looking for leverage.
What else can be optimised around these findings to increase the ability of the detoxification and elimination system to cope effectively with toxins and the immune system to safely and effectively eradicate a pathogen.
How do we get the body (system of systems) into a position where it can function and perform in a more effective way and beyond what it appears capable of currently?
Given the extensive functional medicine assessments we were to run we were confident we would identify some more significant drivers and opportunities for leverage.
Opportunistic Parasite Dientamoeba fragilis

The GI Map Gut Test had yet more markers of interest. Dientamoeba fragilis is not in the classification of pathogen as something like Enterohemorrhagic E.coli. There is indeed some disagreement about whether Dientamoeba fragilis is a serious threat to human health.
Yet the scientific literature certainly supports Dientamoeba fragilis as a potential causative factor in digestive symptoms. Typical symptoms include bloating, gas, loose stools, diarrhea, abdominal tenderness, pain, cramping, fatigue, nausea, weight loss or gain. D. fragilis has also been isolated from surgically removed appendices (after appendicitis), suggesting that the infection may be related to this too.
Importantly, we had the context of the HUS concern, which means that every other finding needs to be interpretated alongside this finding.
If Chloe only knew about the parasite, or was compartmentalising the results, and wanted to eradicate it, she would run the risk of causing more serious damage to her body.
That’s one reason we like to be comprehensive in our assessments at the Functional Health Clinic.
Microbiome in Context and Proportion

We’ll keep the microbiome section purposefully short. There is no doubt that there is more and more fascinating research, funding, testing, writing, training, strategies, interventions, etc related to the trending topic of the ‘microbiome’.
This has many benefits and can be of great value of course.
Yet, there are many drawbacks to this too. The myopia, infatuation and minutiae related to the microbiome seems often to be as much a distraction than of real value towards the ultimate goal – the individual person’s health goal!
For example – it is rarely acknowledged that when there is a significant lack of Intestinal Permeability integrity, probiotic products themselves can end up being an additional immune stressor (triggering Neutrophil infiltration). An actual driver of a continuous and chronic inflammatory response that never gets resolved!
If it can contribute to progress, then great. But if not, then it requires a grounded and balanced approach. Not a ‘this-for-that’.
For Chloe, it was clear that these markers of dysbiosis and depletion in the microbiome’s commensal bacteria was relatively useful. Yes, it could relate to some reasons why she had some of these challenges and solutions to them.
She had taken several courses on Antibiotics during the months in the lead up to the onset of her UC symptoms 18 months ago.
But, there was no real evidence that these should be put in pole position in order of importance and priority.
We also often find that the focus and modulation of other factors will be effective in creating more balance in the microbiome, rather than a direct focus on probiotic/prebiotic/postbiotic foods and supplements.
Immune Eosinophil Activation Protein Very High

This is a relatively new addition to the GI Map profile. ‘The accumulation of Eosinophil Activation Protein in the intestine is associated with inflammation and tissue damage, and the level of EPA in the stool can serve as an objective measure for chronic inflammation in the GI tract.’
‘In the case of inflammatory bowel disease, the marker can be used to evaluate disease activity and predict relapse. The EPA marker can also be used to determine the effectiveness of a food elimination diet to control symptoms or disease progression.’
Associated with Elevated Eosinophil Activation Protein:
- Respiratory allergies
- Asthma
- Food allergies and sensitivities
- IBD
- IBS
- Intestinal parasites
- Eosinophilic esophagitis (EE)
- Functional dyspepsia
- Acid reflux
- Intestinal barrier damage/dysfunction
- Anxiety (IBS-related anxiety)
Of course, some of the identified Pathogens could be significant. But as part of Chloe’s Functional Health Program we knew we needed to start to screen and identify any further factor(s) that could be causing such an immune response in the gut.
It didn’t take long before we felt we had another prime suspect.
Mold!
Calprotectin Inflammatory marker High

Chloe’s Gastrointestinal Doctors had already been monitoring this and her past 4 tests had been high. So this marker on the GI Map was of no surprise. Yet, still of course very important.
Whilst giving context to the value of her Steroid and Biologics medication it also raises the question of whether there are any other factors and pieces of the puzzle that are driving the inflammation levels in her gut? E coli for one.
Intestinal Permeability – High Zonulin
Zonulin is a marker of Intestinal Permeability. The gut membrane (or mucosa) is a barrier that is designed to allow ‘good’ stuff through and stop ‘bad’ stuff from getting through into the blood stream.
The interface.
When the integrity and function is compromised by stress chemistry, damage and inflammation, this ability begins to falter. Dysfunction of this barrier is believed to initiate immune dysfunction because it allows macromolecules from the gut lumen to pass into the bloodstream.
Intestinal permeability, also known as “leaky gut,” has been associated with inflammatory bowel disease, celiac disease, food allergy, irritable bowel syndrome, critical illness, autoimmune diseases, obesity and metabolic disease.
If IBD and Ulcerative colitis are related to autoimmune mechanisms then we’re very interested in an ‘intestinal permeability’ that could be driving and intensifying it further.
So we added this to the list of priorities!
Building a Picture – Ulcerative Colitis and Biologics and Beyond
We were beginning to build a picture. Yet, it can be challenging to get such insight, sometimes overwhelming. But, that’s the other part of the coaching here at the Functional Health Clinic. We know it’s as much about the ‘how’ and ‘why’ as it is about the long lists of ‘what’.
Running testing doesn’t magically solve health challenges. Yet the insight can play a hugely valuable role in the process you are putting in place.
The more clarity you have the more we can do two key things:
1 – Individualise
2 – Prioritise
Believe it or not but most people who contact us can barely identify any individual factors or findings about their health challenge or identify what is a priority to focus on.
Individualising and Prioritising really just highlights where the leverage is.
If we can enhance these two things then we are moving away from the generic, one-size-fits-all approaches and towards an empowered and focussed position.
With that in mind, we also know that in complex cases, we really need more insight than just one great gut test.
In fact, sometimes we are really only scratching the surface of what is going on in the body!
That’s why we did further testing and digging.

We’ve created the stages and phases of the Health Restoration Program so that we can coach our clients a Process. There are so many aspects to share (Principles, Assessments, Strategies and all the why’s and how’s), that we have a structure and framework in place in which to teach each step.
A Comprehensive and Illuminating Blood Chemistry
So what else did we uncover?
We run a Functional Analysis of a Blood Chemistry with every single person we work with. You can read more about the Functional Analysis here:
https://functionalhealthclinic.co.uk/functional-blood-chemistry-analysis/
One of the practical and logistical elements of this is ensuring that it is as comprehensive as possible and reasonable.
Chloe already had a recent blood test from her Doctors, but it was focussed on a small set of markers/panels. As is often the case it was missing a comprehensive Thyroid Panel, Vitamin D, B12, Folate, full Iron Panel and Lipid Panel.
Therefore, Chloe requested to run another more complete blood test, which had some brilliant insight for us.
The ‘Functional’ approach to a blood chemistry does not replace the Medical or ‘Conventional’ interpretation or advice. That remains of paramount importance. The functional remit is simply different. The focus is on mechanisms, how they are performing, considering the drivers, looking for patterns, identifying what could optimise it.


Diminished Liver Function
It really looked like the Liver, which is important for many functions (including detoxification, blood sugar balancing, digestion), was struggling. The blood chemistry showed quite a significant group of markers here. Specifically the outside-of-optimal markers:
- Albumin High
- LDH High
- AST High
- GGT Low
- Iron High
And this may be of no surprise given the finding of Enterohemorrhagic E coli which has been linked to liver inflammation, Non Alcoholic Fatty Liver Disease and Liver Abscesses!
Hence – There are many strategies (nutrition, environment, behavioural etc) that could be valuable here.
But this is where one factor became of clear importance……Mold.
Mold and Water Damaged Buildings
Earlier we highlighted the link between the immune Eosinophil cell marker and Mold. Let’s expand on this.
Whilst this is not about being able to state what caused Chloe’s medically diagnosed condition – this is about identifying what could be causing damage, stress and inflammation in her body.
This may not always be about identifying the original driver and more so be about what is perpetuating the chronicity.
About 1 year prior, Chloe and her family had moved house into a relatively new build. Due to the layout of the house, the bedroom was downstairs where there was evidence of damp and they could see and smell mold in both the bedroom and bathroom.
Right away we knew that Mycotoxins may be an important piece of the puzzle for the whole family. Especially because of the fact that the bedroom was implicated. Significant due to the duration we spend in this room and how much of an impact that can have.
‘The topic of Mold, Mycotoxins and Chronic Inflammatory Response Syndrome (CIRS) is potentially vast and valuable. Building and Body Assessment and Remediation is sometimes required on a comprehensive level.
But we wanted to see what we could review and modulate relatively quickly and practically.
They started to make changes with some actionable steps.
Better ventilation and a good quality Dehumidifier.
Mold – Immediate Changes
This was actually one of the first changes we coached to Chloe. It was deemed such as priority that she started immediately after her Initial Consultation.
By the time we spoke again on her next consultation two weeks later, she was already improving.
Her dry, sensitive and itchy eyes had already completely cleared up!
The dehumidifier in the bedroom was collecting a lot of water at on the 80-90% setting
After a few weeks it was eventually down to about 60% and needed much less frequent emptying.
In the meantime, they had also had the roofing investigated and found that the insulation had been poorly done previously and was the probably cause of creating such conditions and environment in the house.
Mycotoxins and Vitamin B12
The Lab that runs our MycoToxin tests explain that “Mycotoxins, produced by certain mold species, are some of the most prevalent toxins and can come from many sources, including buildings, vehicles, and food. These compounds have been recognized as a growing global health concern due to their acute and chronic adverse health impacts.”
https://mosaicdx.com/test/mycotox-profile/
People exposed to mycotoxin-producing molds commonly also present with a vitamin B12 deficiency that is unrelated to diet. There is some evidence to suggest that mycotoxins may interfere with the metabolic pathways that regulate Vitamin B12.
https://pubmed.ncbi.nlm.nih.gov/17982599/
We can see from Chloe’s blood test that her B12 was outside of the optimal range.
Her Hair Mineral Test also indicated a potential Vitamin B12 deficiency behind the scenes of the blood chemistry. We can see her low Cobalt level here which relates to cobalamin (vitamin B12).


Fast forward to a retest and we were able to increase Chloe’s Vitamin B12 Blood Test level to optimal.

Mycotoxins and IBD / Ulcerative colitis
Could it be that one of the major drivers or ‘stressors’ involved in the inflammatory bowel disease and/or the difficulty in creating a resolution was the Mold and Mycotoxins?
We probably can’t answer that. The work we do is too multifactorial, to be able to point at one single thing and say ‘that caused everything!’
That’s not really our focus.
But it seems clear that this was at least a very significant piece of the puzzle.
Here’s another interesting Case Report of Chronic Inflammatory Responses and Biotoxin Exposure: https://pmc.ncbi.nlm.nih.gov/articles/PMC4913732/
There are some very specific and clear links in the research as to how this could be affecting Chloe’s intestinal lining, permeability, immune function, inflammation levels and toxic burden!
Here’s a very interesting paper: ‘The Compromised Intestinal Barrier Induced by Mycotoxins’
“In addition, intestinal perturbations caused by mycotoxins may also contribute to the development of mycotoxicosis, including human chronic intestinal inflammatory diseases.”
So now we have more insight, clarity, action steps, feedback and progress.
Iron Intricacies
Whilst we are reviewing the Functional Blood Chemistry Analysis, let’s take a moment to look deeper into Chloe’s Iron status.
‘Iron’ is a fascinating topic for us. We’ve learnt so much about it in the last decade in particular.
It is of course an incredibly important mineral, but one of the major challenges is how it is conventionally assessed and interpreted.
It seems that most of our clients have only ever run a ‘Ferritin’ test with their Doctors.
Rarely has there been a Full Iron Panel that would ideally include markers such as:
- Iron
- Ferritin
- UIBC
- TIBC – Total Iron Binding Capacity
- Transferrin
- Transferrin Saturation
The Blood Count Markers can also be very insightful, such as:
- Haemoglobin
- Haematocrit
- Red Blood Cells
- MCV
- MCH
- MCHC
Here’s a very helpful review of these Iron markers: https://www.rupahealth.com/biomarkers/iron
Given the full potential for insight with this range of markers, we really endeavour to do more than just look at Ferritin.
Ferritin does have value as a marker of iron-storage protein, providing some indication of available iron stores. An increased ferritin level can be associated with excessive iron storage (e.g. haemochromatosis), iron poisoning, recent blood transfusions, megaloblastic anaemia (anaemia due to vitamin B12 or folic acid deficiency) or haemolytic anaemia (anaemia caused by premature destruction of red blood cells). Decreased ferritin levels can be associated with iron-deficiency anaemia and very low protein levels.
However, the disadvantage it as an interpretation of iron status is this.
Ferritin is an acute phase protein.
This means it can increase with acute inflammatory disease, infection, liver disease or cancer, due to leakage of ferritin from damaged tissues/organs (especially the liver, spleen and bone marrow).
Which is unrelated specifically with actual Iron stores.
Chloe’s ‘Low Ferritin’
Historically, the Drs Ferritin Test would always come back Low.
This seems like an important finding. But what is it actually indicating? From a functional perspective, this would certainly warrant some further assessment and investigation.
At that point Chloe was not running a full Iron Panel, yet the result was deemed to indicate Low Iron levels.
So by the time we met, Chloe had already received several Iron Infusions.
Once we started work, we ran the Comprehensive Blood Chemistry, which included a full Iron Panel and we actually found:
Iron – High
Can be associated with disorders of excessive iron storage (e.g.haemochromatosis), iron supplements, blood transfusions, haemolytic anaemia, lead toxicity, and liver or kidney disease.
Ferritin – Normal
Transferrin – Normal
Transferrin Saturation – High
An increase can be due to disorders of excessive iron storage (e.g. haemochromatosis), increased iron intake or other types of anaemia, such as haemolytic anaemia and megaloblastic anaemia (anaemia due to vitamin B12 or folic acid deficiency).
Bringing more focus to her established Low Vitamin B12 levels.
The Blood Count Red Blood Cells were all in the Optimal Range. This was great to confirm given how this could otherwise relate to the above causes of the iron imbalances.
We referred Chloe to her Doctors regarding and further medical work-up and genetic screening for Haemochromatosis.
Given that the prior iron infusions are likely to have impacted these markers, it appears that if there was previously an ‘iron deficiency’, then this wasn’t the case any longer.
Assessing and monitoring the markers empowers the ability to adjust the intervention as appropriate. In this case it could inform her Doctors about dosage/timing/requirement of her iron medication.
Now, this was even more important given the emerging pattern of an increase in symptoms in the days following her Iron Infusions.
The risks associated with Iron Excess are significant. Different, yet as challenging in nature as Iron Deficiency.
Given the additional consideration of kidney health and HUS, then the fact that “Intravenous iron can cause oxidative stress, which can lead to proteinuria and tubular damage in the kidneys” would be a concern.“ https://www.sciencedirect.com/science/article/pii/S0085253815499739
Improving Iron
We knew we needed to monitor this throughout the whole process and 5 months later we ran another Blood Test.
Unfortunately the blood sample haemolyzed at the lab so they couldn’t test the Full Iron Panel. But her Iron level was moving back towards optimal levels, Ferritin was still Normal, Red Blood Cell markers still Normal and the B12 had optimised.
Chloe shared and discussed this progress with her Doctor and decided to stop the Iron Infusions too.


Let’s take a look at some of the other interesting themes, factors, experiences and strategies that we encountered throughout the Health Restoration Program.
Steroids and Dental/Oral Health
After stopping her Steroid medication a few months earlier, her teeth and gums had become very sensitive and sore.
Here’s an interesting description of the Prednisolone (steroid) medication which had been prescribed to treat the IBD:
“Prednisolone is a synthetic corticosteroid drug that is particularly effective as an immunosuppressant drug. It is used to treat certain inflammatory diseases (such as moderate allergic reactions), some autoimmune diseases, and (at higher doses) some types of cancer, but it has significant adverse effects.
The dental-related side effects due to steroid that had been studied include pulp chamber and root canal obliteration and root resorption during orthodontic tooth movement under the effect of corticosteroid. Corticosteroid treatment has also been shown to interfere with orthodontic tooth movement rate and tissue reaction.”
https://pmc.ncbi.nlm.nih.gov/articles/PMC6385580/
This doesn’t completely describe and explain Chloe’s experience having the oral and dental symptoms increase when coming off her steroid prescription. But certainly highlights some of the mechanisms, functions and tissues that are affected.
It helped us target and focus on some changes to her routines and strategies to support her dental and oral health.
This may have also simply have been a process of time-passing and more restoration for Chloe, but by the end of our work together this is another health challenge that had completely alleviated.
Hair Loss
Her increased rate of hair loss had been occurring for the previous six months when we first started working with Chloe.
Over the next few months we were able to eventually alleviate this completely.
But this isn’t a ‘hair-loss treatment’ program, so how was she able to be so successful? Let’s look more closely at some of the factors involved.
As per any sign, symptom or condition – the functional health approach considers the drivers/causes to be fundamentally individual and multi-factoral in nature.
Whilst it is sensible to assess and approach the well-known and conventional connections, it is wise to consider any of the psychological, physiological and physical aspects.
Hormones and Hair Loss
The jury really is out on causes of hair loss. The conventional idea is that one of the mechanisms involves an increase in testosterone that affects the hair follicles, minimizes them and leads to hair loss. This in itself is questionable because testosterone is a steroid hormone and typically causes growth of tissues, not destruction and the mechanism hasn’t actually been proven.
In really simple terms it is interesting to view the cause of hair loss as an increase of ‘anti-hair’ hormones and a decrease in ‘pro-hair’ hormones.
This imbalance often occurs due to the physiology of the ‘stress response’ and the inefficiency of our body’s cellular metabolism.
So a great stress load leads to more anti-hair hormones like cortisol and adrenaline being produced. And a strong metabolism requires the likes of pro-hair hormones like Thyroid, progesterone and DHEA in order to heal and grow tissues.
Many of the changes that Chloe implemented would have significantly influenced these levels.
Thyroid Function and Hair Loss
The thyroid-connection is well established and is one of the key reasons why a comprehensive blood chemistry that includes comprehensive Thyroid markers is important in our Health Restoration process.
The Hair Mineral Analysis pattern of lower thyroid function and the blood chemistry Low T4 were really valuable insights.


Nutrients, Metabolism and Hair Loss
Macro and Micro nutrients will also have an affect on our metabolism. For example, pro-hair nutrients include optimal proteins, fats and carbohydrates, Vitamin D, E, K, A, Selenium, Calcium, B6, Zinc, Copper, B12 among others.
Testing for Nutrient levels is not always straight forward.
What we aim to do at the Functional Health Clinic is to squeeze the value out of the testing and assessments that we have available.
‘Healing’ is not about running every test under the sun!
One way we do this is to look for patterns across different tests. Afterall they may be different tests, using different samples and being analysed by different labs.
But……….They all have something in common.
They are all providing feedback and insight about ‘you’. The individual. A system-of-systems.
The brilliant combination of a Hair Tissue Mineral Analysis alongside a Comprehensive Blood Chemistry provided interesting insight regarding Chloe’s ‘pro-hair’ nutrients:
Low Vitamin D
Low Selenium
Low Copper
Low B12
Low B6
This information can be used to carefully target specific nutrients, but also to prioritise other areas/functions that would help improve the status of these nutrients. Namely nutritional choices, bioavailability, digestive capacity, gut health, turnover depletion and more.
Immune Function and Hair Loss
In some cases of hair loss, the immune system is playing a vital role. For example, there can be an inflammatory or autoimmune component.
And in this case study that is well established as a very important consideration and likely one of the connected reasons why the hair loss alleviated.

Individualised Nutrition
In a complex case like this, there will rarely be just one nutritional change, one food or even one diet to follow that will be groundbreaking for the person.
Indeed, if you are reading this as someone who is experiencing gut health challenges, inflammatory bowel or ulcerative colitis, then proceed with caution.
There is no one-size-fits-all.
What works for one person will not necessarily work for the next.
That’s not a convenient saying or phrase. Its fundamental to human nutrition and we prefer our clients not to find out the hard way.
We teach and coach a nutritional process that builds from and on where they are currently at.
That’s the baseline and its valid.
Then, given that it may not be optimised to their individual needs yet, we set about the process of making ‘one’ change at a time.
Whilst we may have a number of question marks over several elements of the diet so far, we avoid the judgement and assumptions.
We let the assessments and the process do the rest.
Each step brings us closer to understanding the applying the nutrition that works for each individual.
Here’s a little insight into the highlights and what helped for Chloe:
There were initially a lot of pulses and beans in the diet and she significantly removed them.
Stopping cooking with olive oil.
High quality lard, butter, coconut oil.
Soy eliminated.
Gluten eliminated.
Not relying on Gluten-Free alternatives.
Breakfast more consistently.
Frequent Carrot salads.
Eliminating chia seeds.
Macronutrient levels fine tuned (carbohydrates, fats and protein).
Quality and timing of coffee.
Mineral Broths
There are quite a few changes here. But what she created was not the ability to ‘follow a diet’. It was the ability to learn what her body thrived on.
Cravings and Perceptions around ‘Fullness’
During the many hours and discussions on nutrition, the topic of ‘cravings’ came up.
It often does and it is one of the most stigmatised topics in nutrition/health.
Chloe had been experiencing them for a while. Yet she would also feel full quickly and at the same time feel unsatiated!
Our functional health approach is to avoid the stigma and judgement and focus on the mechanisms, which saves an enormous amount of time and energy (resources).
If you’ve ever watched a dog chase its tail, you’ll see that it’s going nowhere! With no lack of resources invested. At the end of it all they are exhausted.
The conventional stigma and perception on ‘Cravings’ is that they are wrong, bad etc and shouldn’t be happening and you need to work against them and or suppress them!
A more grounded perception is that they are simply a feedback mechanism. To be put into context and worked with in order to progress towards whatever the person’s goal is.
In the simplest terms, the craving is a feedback mechanism to highlight and bring to our attention that something is missing.
It may be as simple as something sweet or salty, which correlates well with the specific craving, but it is wise to initially consider that there is ‘something’ missing.
The next question is what is this ‘something’?
From a cellular biochemistry perspective this could be mineral and vitamin nutrient(s) or protein, carbohydrate and fat macronutrient(s).
We would benefit from a broader discussion of the interoception function of the brain in explaining the interpretation of the information that is being sent from the cells. Hint – The brain is brilliant and impressive, but it still has it’s limitations!
For Chloe we focussed on how fullness is not the same thing as satiated.
What she had been experiencing as ‘fullness’ and normal for a long time (years/decades) was likely not what her cells considered adequate. Which leaves a void.
Therefore, even after eating a volume of food that triggers stretch receptors in the GI Tract and provides the sensation of fullness and feedback to ‘stop eating’. There is likely a deficit that needs to be addressed.
Hence the cravings.
The simplicity of a craving is that it is noticeable. We quickly become consciously aware of a need to fill a void. It quickly creates a change in our goal and behaviour.
The body has found a way to increase the likelihood of us consuming something that provides what our cellular metabolism is demanding.
It has literally motivated us to take action. To go hand to mouth (prehension).
Whether our skill set of interpretation and tool kit of strategies and decision making capacity is up to the task of coming up is an accurate and congruent answer and action – is another question.
Yet – if we are working with the carvings and not against them, we’ll certainly be empowering this process in the direction of the goal and progress.
Rather than just exhaustively going round and round in circles.
Nutrient Density and Bioavailability
Here are the two nutrition principles that are usually not being met and a key reason why cravings occur and many aspects around nutrition are not full filling.
Nutrient Density and Bioavailability.
The food/diet that any given person will thrive on is as close to optimal for both of these principles.
Not just one and not the other. Both.
If we aren’t achieving this then we are almost guaranteeing a shortfall in nutritional value from the food we eat. A deficit.
Most ‘health’ foods are nutrient dense. The Nutritional Science, Labs, Research and Textbooks have gone a long way to quantify the nutrients in a given food.
But that’s where most people will stop digging and make the assumption that it will work for them.
Bioavailability seems to be the area that is missed by so many.
Consider how bioavailable those nutrients are the body.
Not just as a human, but the individual too.
Please drop us a message if this is something that you would like to look into more.
At the Functional Health Clinic we steer clear of the quest to label foods as ‘super’ or ‘bad’, ‘healthy’ or ‘unhealthy’, etc.
Before we forge on with more details into Chloe’s journey with the Biologic Infliximab medicine, let’s present the progress we made and the results we achieved by the end of the Health Restoration Program.
Health Restoration – Post

This review of symptoms seems almost too good to be true! At the end of a process like this when dealing with chronic and complex we usually and realistically have some challenges that have not fully alleviated and even have the occasional one that has not changed during the coaching program.
What we would say is that, the ultimate goal is for our client’s wellbeing and progress to be robust in nature. Something that has longevity and constitutes a real change.
And when future challenges do arise, we trust that we have added to the skill set of the ability-to-respond!
Now let’s delve into some depth on the intriguing area of her Infliximab Biological Medicine.
The Context of Integrating the Functional Approach
The challenges faced by Chloe’s medical team will have been quite enormous and the work done incredibly valuable, even lifesaving. Yet, the remit is very focussed on these priorities and not outside of them.
From a functional perspective it is still fascinating that there was almost zero investigation into the causes and drivers of the individual’s IBD.
Chloe achieved her progress, in part by asking more questions to find out these answers.
Without this endeavour she identified potential contributing factors such as:
Enterohemorrhagic E coli infection
HUS toxicity and burden.
Mold and Mycotoxins.
Nutrition, Gluten.
Nutrient Deficiencies, eg B12
Nutrient Excess, eg Iron
All of which have a clear and defined role in immune function, autoimmune mechanisms and………IBD.
For us, this demonstrates the value of integrating approaches.
Rather than creating the dichotomy of ‘either/or’.
What about carefully, logically, safely and effectively addressing the individual’s goals, drivers, causes, interventions, solutions and progress?
Ulcerative Colitis and Biologics, Infliximab and Immune Function
This client’s very unique situation and set of goals made for a fascinating scenario.
There were clearly some major health challenges present.
Already a great deal of medical support.
Yet a significant desire to improve and optimise function and vitality.
When we first met, the Biologic, Infliximab Infusions were a significant part of Chloe’s approach to managing her Ulcerative colitis so far. Along with the steroids that she had recently stopped.
But Chloe had felt that the impact had come from the steroids, was unsure about how much the Infliximab was supporting her body and was concerned with the ongoing and long-term implications.
Chron’s and Colitis UK: “Infliximab belongs to a group of medicines called biologic medicines. Biologic medicines are made by a biological rather than a chemical process. They’re produced in a lab by living cells.
Infliximab is an antibody-based medicine. It targets a protein in the body called tumour necrosis factor-alpha (TNF-alpha). TNF-alpha is naturally produced by your body and helps fight off infections. Too much TNF-alpha can damage the cells that line the gut. This may partly be the cause of gut inflammation for people with Crohn’s or Colitis. Infliximab binds to TNF-alpha, blocking its harmful effects, which reduces inflammation. This can help to relieve symptoms.”
Whilst all of the remit and role around Chloe’s Ulcerative Colitis and Biologics Medication and treatment of her medical condition was the for the NHS and her Medical Team – it was still important for us to understand the mechanisms.
Which is where the Functional Immunology comes in.
We also consider that there may of course be some drivers of the inflammation.
Reasons for the TNF-a production to be elevated.
Afterall – the Inflammatory response is a natural and normal function of the immune system. Part of the blueprint.
Whilst high and chronic levels of the inflammation are clearly not desirable, are serious and may often require significant management and interventions – these causes of the inflammation could actually be pivotal.
Even, at the very least, if identifying and modulation drivers of inflammation would aid a reduction of symptoms of IBD, increase the quality of life and require less Medical management and intervention, then it seems valid.
So, it seems wise to consider what these factors could be.
For example – pathogen, food, allergen, toxin etc.
At the Functional Health Clinic we focus on this so that we can Individualise and Prioritise and create safe and effective strategies that are congruent with the person’s goal.
Immune Th1 vs Th2 cells
The Functional Immunology work we have studied and apply with our clients is often quite unique to their journey so far.
We regularly discuss the Th1-Th2 Seesaw as this is where there are some significant patterns and imbalances.
Many immune/inflammatory based disease processes will be dominant in one side or the other of the T-helper 1 cells or the T-helper 2 cells.
Th1 cells respond to intracellular bacteria and some viruses, whilst Th2 cells respond to ‘stressors’ in the hollow spaces (eg GI Tract, Oral Cavity, Urinary Tract).
Whilst both are Inflammatory Bowel Diseases – Crohn’s Disease is considered Th-1 Dominant and Ulcerative Colitis is typically considered Th-2 dominant.
Even within IBD, different parts of the immune system are driving different inflammatory responses.
So theoretically, this would mean that the goal in Ulcerative Colitis is to identify the drivers of the higher Th-2 response and dampen it and consider support to lift the Th1.
Infliximab targets and reduces TNF-alpha as it is considered to be driving some of the inflammation in UC. But TNF-alpha is also involved in the Th1 cell immune response, so this medication may also contribute to a further lowering of this side of the seesaw too.
Whilst at the same time as providing some anti-inflammatory support, could this also be creating a further skew and polarisation in the immune system?
Are there additional steps that can be taken to see it the high Th2 and low Th1 activity levels can be brought back to balance?
It isn’t clear whether this is taken into consideration with long-term prescriptions for patients.
Infliximab over Long-Term
In fact there is some interesting research that demonstrates that in some scenarios, there may be opportunities to actually titrate down the Infliximab dosage.
Given that long-term usage could lead to significantly low white blood cell levels, which could lead to a vulnerability to other infections.
https://bmcmusculoskeletdisord.biomedcentral.com/articles/10.1186/1471-2474-13-184
“In conclusion, our study demonstrated that measuring infliximab serum trough levels and anti-infliximab antibodies during the maintenance phase of infliximab treatment could be of value to optimise treatment. Low (and to some extent high) infliximab serum trough levels are prevalent in RA patients treated for a longer time with infliximab, also in patients with low disease activity. Since infliximab serum trough levels and anti-infliximab antibodies are reliable measurements, these might be used to identify patients in whom infliximab can be de-escalated or stopped.”
There was a point during Chloe’s Health Restoration Program that she was due to get her next Infliximab Infusion.
Interestingly, she seemed to fit the profile of when it may be appropriate to consider a potential titration down of her Infliximab Medication.
Yet this was a matter for Chloe and her Medical Team to discuss.
The value of her Biological may have been quite remarkable, but she also wanted a plan and a process in place for the bigger picture and the future.
“Double Your Dosage”
It is fair to say that Chloe was a little surprised to hear that her Consultant simply wanted to Double her Dosage.
They advised four more double dosage infusions over the next few months before running any further blood tests.
The main driver for this decision was that her Infliximab levels were too low. “Usually’, this would mean that the Infliximab may not be effective enough to control the inflammatory process.
The levels were so low that her Specialist Team stated that they would have expected her symptoms to have been on the increase and quite severe – not improving as they actually were.
Informed Choice and Balanced Decision Making
This was a complex scenario for Chloe to navigate. On one had she was experiencing improvements in vitality and could see the benefit of the medical and functional strategies in place. And on the other, in real time, she needed to continue making decisions that were congruent with the dynamic nature of her body and her goals.
To emphasise, whilst we deliver a ‘Functional’, not Medical approach, there is no bias for or against Chloe’s approach and decisions around her medical diagnosis of Ulcerative Colitis and Biologics Medication prescription. The aim is for the practitioner (us) to also stay informed and clear as to what our client is putting in place.
On asking a few questions to her Specialist Team, she was initially told that she could only speak to the Consultant in 3 months time after the next few Infusions at a double-dosage.
Chloe was also told that the level of dosage made no difference to any side-effects! This is something that appears to require more explanation.
Chloe felt at that point that she was getting a general response so raised some further points related to her individual case. Thankfully her Consultant responded to this and managed to schedule her in that week, prior to her next infusion and they agreed to maintain the current dosage and monitor carefully.
After a few more weeks of sustained progress Chloe discussed with her Dr and chose to stop the Infliximab Biologic.
It was certainly a challenging transition, that took a lot of careful steps and monitoring. But by the end of her Support Program she was had been Medication-Free for several months and her health was improving week-by-week.
Chloe also followed-up with us at the point of being 12-Months Medication-Free, reporting further improvements to her vitality and no occurrences of IBD or Ulcerative Colitis.

Challenges Along the Way
There is no rose-tinting a journey like this.
The process is never linear and continuously improvement after improvement and without its challenges.
At every step there is a decision to be made. Another area to become more informed and grounded in in order to make the decision that is congruent with the direction you are wanting to head in and the goal you are looking to achieve.
For Chloe, she was exhausted, raising a 1 year old that was struggling to sleep at night, returning to work after maternity leave and was experiencing stress in her relationship.
And because nobody lives in a bubble – the things you don’t plan for, but are part of the process such as Norovirus and food contamination.
Realistically – these are simply part of the process.
The Ability-to-Respond to every challenge is what we maintain the focus on.
We apply the principles of human function (and behaviour) to all the steps and instances along the way.
Not just when it’s easy or convenient.
We put a large part of Chloe’s progress down to the ‘Why’ and the ‘How’ as much as we do the ‘What’.
Considering the Stages of the HRP – after the first few months, digging in and ploughing through the Foundation and the Grounding Stages, Chloe was definitely firmly into a Rhythm. The ups and downs would demand that we returned to some prior stages, but by the end of the process there was a sense of Flow and robustness to what Chloe’s Vitality.
The creative process she put in place to create clarity and navigate her way towards her goal was inspiring to observe.
Chloe’s Full Testimonial
Unfortunately, during this treatment I had multiple colitis flares, and extensive progression with my IBD, especially after the birth of my daughter. I had trialled, oral courses of Oral Steroids, Mesalazine, Azathioprine and then combined with steroid suppositories, all of which didn’t help. My symptoms worsened, and in the space of 18 months, I had 2 hospital admissions for severe acute flares, 1 admission for pancreatitis (caused by Azathioprine), side effects from the steroids, IV pain relief & anti-emetics. I was told on my last Medical admission, that unfortunately this is the nature of the disease and one day I will most likely become that poorly, I would need bowel surgery for a colostomy. Therefore, I decided to try Biologics, a popular and often last resort medication choice for IBD symptom management. I received regular IV infusions of Infliximab and again, this medication doesn’t come without its side effects and unfortunately, it wasn’t clear how much the infusions were helping. After experiencing, constant fatigue, bloody diarrhoea, urgency, abdominal discomfort and disturbed sleep due to bowel movements, I lost all hope. Most importantly felt robbed of my motherhood whilst trying to battle this cruel disease. I spent more time trying to manage my disease, than I did looking after my baby. I started to research ulcerative colitis further, looking for other options and I discovered the functional health approach. I worked with Jack for around 12 months. He took an extensive history and we started the work from there. We ran a multitude of tests and started to identify the factors and results which were likely affecting and worsening my colitis. And even factors which could have been an initial cause. Before we started the work, Jack made it clear that this wouldn’t be an overnight fix and it required consistency and effort. I was surprised at how many aspects of my life, if not all, we discussed. From food, to triggers, medication, environmental factors, relationships, stress chemistry, supplements, sleep etc, the list could go on. I never realised that all the above could be influencing my disease. I made the choice, to stop my Biologics, and was able to smoothly come off this medication with Jack’s remit being to support the functional health side of things. We identified certain triggers over the last 12 months, the small flares within this time became shorter, faster to overcome and I was able to resolve these without the need for a course of steroids, which had never happened before.I finally felt like I was healing my gut. Making progress without the need to just manage it and with no medication required. My inflammation markers, continued to reduce over the 12 months. I am now in a position, where I no longer suffer from my symptoms of 18 months ago. The extensive tests Jack ran, reflect the huge improvement in my gut health. The knowledge gained is invaluable. I will forever be grateful, for the help Jack has provided me over the last 12 months. I would recommend functional health to anyone struggling with their own health, as it has truly changed mine. Thank you Jack
Gut Health

CBC

Organic Acids
